You’re sitting in the dentist’s chair, nodding along to the familiar flossing lecture you’ve been politely ignoring for most of your adult life. Fair enough. It’s hard to get excited about gum health. But it turns out your dentist may have been underselling the pitch.
A study published in January 2026 in Cell Communication and Signaling shows that a common gum disease bacterium can promote breast cancer growth and spread in mice, and the findings hint at a particularly troubling link for people carrying BRCA1 mutations (1). “Floss to help prevent cancer” probably wasn’t on your 2026 bingo card, yet here we are.
Platelets are best known for their role in blood clotting, but they also participate in other biological processes that influence how cells communicate and behave. In research models, scientists have observed that tumor cells can interact with platelets in ways that affect how they move and attach to new environments. A recent study by Morris et al., published in Scientific Reports, explored the molecular details behind these platelet–cell interactions and the role of calcium in regulating them.
The Role of Integrins and Calcium
The study focused on integrins, which are surface proteins that help cells anchor to their surroundings and communicate with the extracellular matrix. Two integrins, αIIbβ3 and αvβ3, are particularly important because they mediate platelet–platelet and platelet–cancer cell binding. Their structure and function depend on divalent cations such as calcium, which stabilize receptor conformation and support ligand binding.
When extracellular calcium levels were manipulated, platelet behavior changed in distinct ways.
T cell-based immunotherapies, including CAR-T and TCR-T therapies, have transformed cancer treatment. T cells are a type of white blood cell that plays a central role in the immune system, recognizing and eliminating abnormal or infected cells. These therapies train T cells to attack tumors; however, a major hurdle remains: most lab-grown T cells fail to persist after an infusion in a patient. Despite transferring millions of tumor-targeting cells, many quickly die off, limiting their effectiveness inside the body. But why?
Discovered in 1983 and initially dismissed as ‘cellular dust,’ exosomes have since emerged as pivotal players in biomedical research due to their roles in intercellular communication, potential as drug delivery vectors and as biomarkers for various diseases. These small extracellular vesicles, measuring 30–150nm, are crucial for transferring proteins, lipids, and nucleic acids — including microRNA (miRNA), mRNA, and non-coding RNA– between cells (1). miRNAs are particularly critical as they regulate gene expression and offer insights into the cellular mechanisms underlying diseases like cancer, enhancing the value of exosomes in cancer research.
Beyond exosomes importance in understanding intracellular communication and organ cross-talk, exosomes can also alter the functions of recipient cells based on their cargo. This capability makes them extremely valuable in providing insights into alterations in cellular communication, tumor microenvironments, metastasis and immune evasion.
Chimeric Antigen Recepter (CAR)-T cell therapy is a personalized immunotherapy that harnesses the patient’s own immune system to combat cancer. It is done by engineering the patient’s T cells to specifically target and attack cancer cells in their body, and it has shown great success in treating various blood cancers such as leukemia.
Treating solid tumors with CAR-T cells, however, has proved much more challenging. This is mainly because solid tumors contain a heterogeneous population of cells, expressing a variety of antigens—many of which are also expressed in healthy cells. Therefore, T cells targeting solid tumors could potentially attack healthy tissue, resulting in serious side effects. In addition, solid tumors create a hostile microenvironment that is difficult for CAR-T cells to infiltrate.
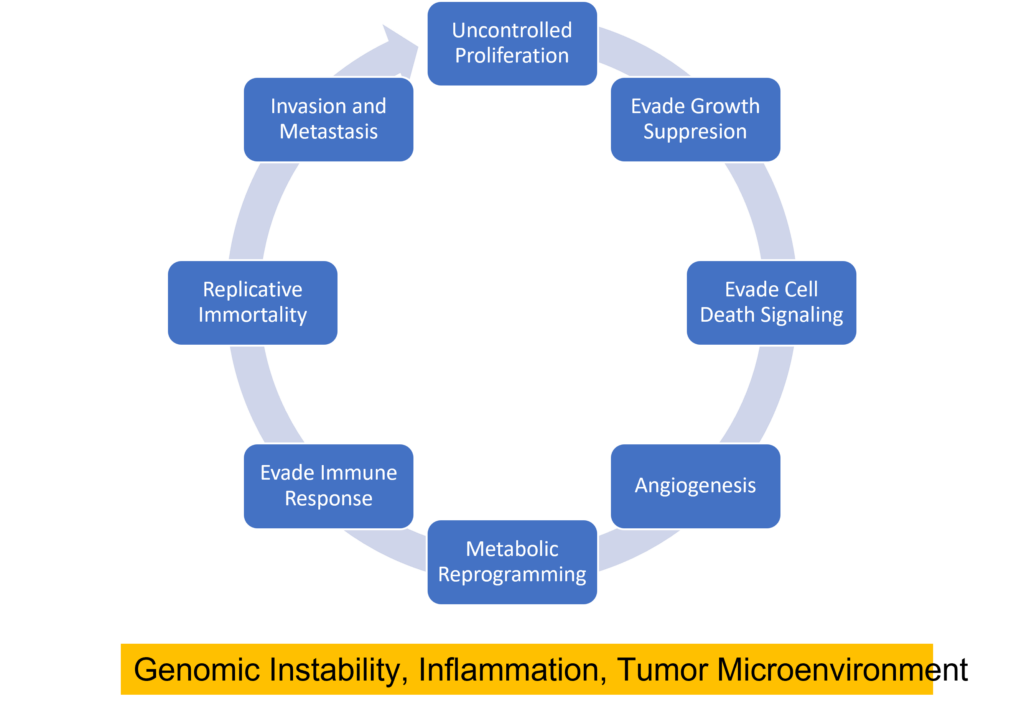
Cancer cells can be distinguished from normal cells by a variety of features including their ability to inappropriately activate signals for cell proliferation, evade growth suppression from contact inhibition or tumor suppressor activity, evade cell death signals, replicate DNA continually, induce angiogenesis, invade new tissues, reprogram their metabolism to provide energy for rapid proliferation, and evade immune detection (1) . Several biological processes are responsible for these features including genomic instability, inflammation, and the creation of a tumor microenvironment.
The tumor microenvironment is the network of non-malignant cells, connective tissue and blood vessels that surround and infiltrate the tumor. These surrounding “normal” cells interact with each other and the cancer cells and are important players in tumorigenesis. One cell type that is often found in the tumor microenvironment are nerve cells. In fact, cancer cells often express proteins that encourage nerve growth into the tumor microenvironment such as growth factors and axon-guidance molecules (2). Crosstalk between nerve cells and tumor cells can facilitate development of several cancer types (2) including pancreatic, head and neck, oral, prostate, and colorectal cancers.
Centrosaurus is a herbivorous Ceratopsian dinosaur that lived in Canada in the Cretaceous Period.
Did dinosaurs get cancer? That isn’t an easy question to answer. Finding and diagnosing cancer in dinosaur fossils has proven difficult. Any soft tissue, the typical location of tumors, has degraded over the millennia. Fossilized bones millions of years old are subject to wear and tear, making it hard to distinguish bone damage from possible pathology. By using the knowledge and expertise gained from diagnosing cancer in humans, a team reported in The Lancet Oncology that they found the first known case of osteosarcoma in a lower leg bone from a horned dinosaur found in southern Alberta, Canada.
This case of bone cancer discovered in a specimen of Centrosaurus apertus found in the Canadian Dinosaur Park Formation was confirmed by examining the bone surface along with radiographic and histological analysis. The 77–75.5-million-year-old case was compared to both a normal C. apertus fibula from the Oldman formation also in southern Alberta, Canada, as well as a human fibula with an osteosarcoma.
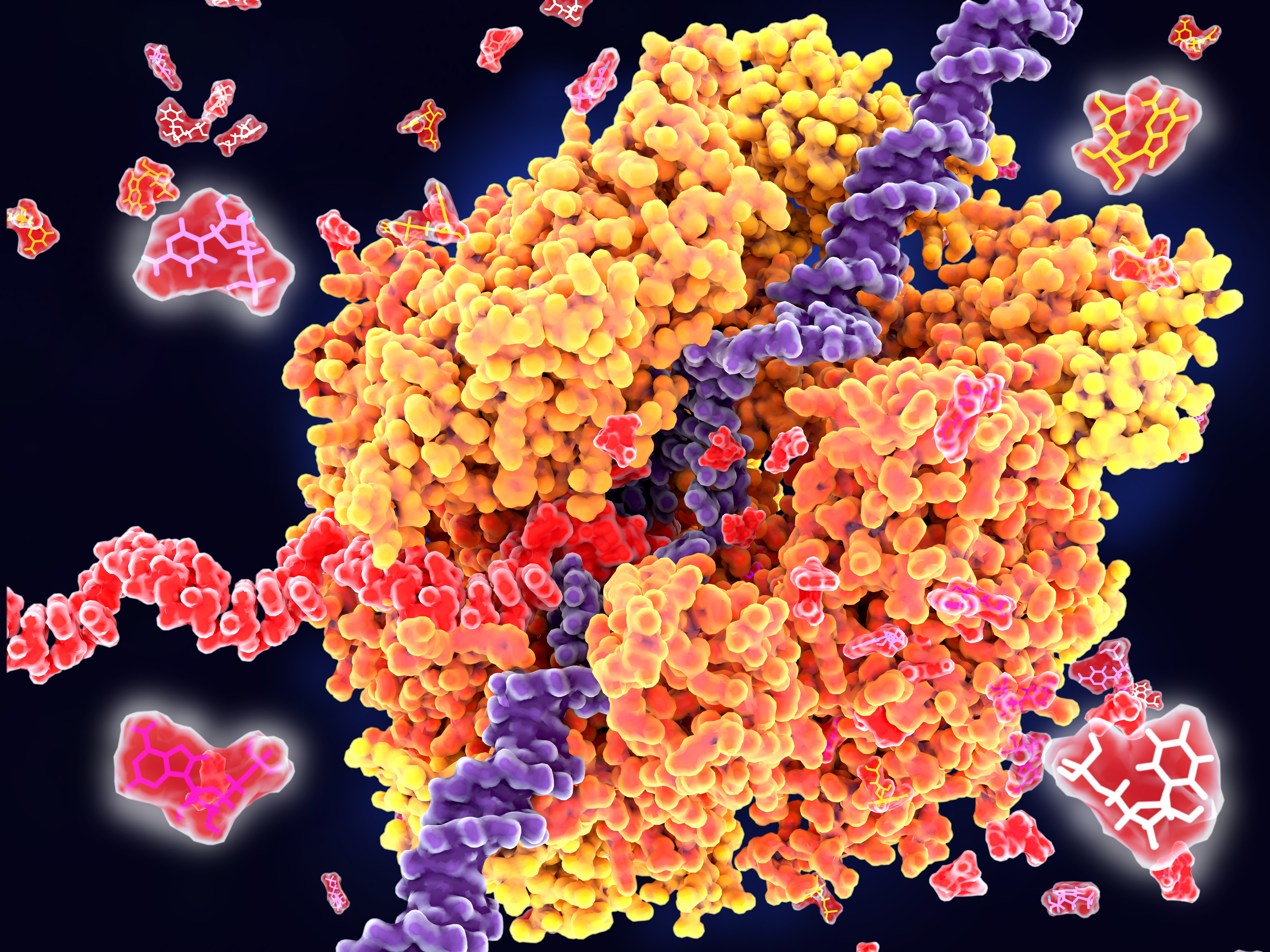
RNA polymerase unwinds DNA strands for transcription.
Transcription is the production of RNA from a DNA sequence. It’s a necessary life process in most cells. Transcription performed in vitro is also a valuable technique for research applications—from gene expression studies to the development of RNA virus vaccines.
During transcription, the DNA sequence is read by RNA polymerase to produce a complimentary, antiparallel RNA strand. This RNA strand is called a primary transcript, often referred to as an RNA transcript. In vitro transcription is a convenient method for generating RNA in a controlled environment outside of a cell.
In vitro transcription offers flexibility when choosing a DNA template, with a few requirements. The template must be purified, linear, and include a double stranded promoter region. Acceptable template types are plasmids or cloning vectors, PCR products, synthetic oligos (oligonucleotides), and cDNA (complimentary DNA).
In vitro transcription is used for production of large amounts of RNA transcripts for use in many applications including gene expression studies, RNA interference studies (RNAi), generation of guide RNA (gRNA) for use in CRISPR, creation of RNA standards for quantification of results in reverse-transcription quantitative PCR (RT-qPCR), studies of RNA structure and function, labeling of RNA probes for blotting and hybridization or for RNA:protein interaction studies, and preparation of specific cDNA libraries, just to name a few!
In vitro transcription can also be applied in general virology to study the effects of an RNA virus on a cell or an organism, and in development and production of RNA therapeutics and RNA virus vaccines. The large quantity of viral RNA produced through in vitro transcription can be used as inoculation material for viral infection studies. Viral mRNA transcripts, typically coding for a disease-specific antigen, can be quickly created through in vitro transcription, and used in the production of vaccines and therapeutics.
In 2012, a 6-year-old girl named Emily Whitehead was battling acute lymphoblastic leukemia (ALL), one of the most common cancers in children. Her cancer was stubborn. After 16 months of chemotherapy, the cancer still would not go into remission. There was nothing else the doctors could do, and she was sent home. She was expected to survive only a few more months. Her parents would not give up and enrolled her into a clinical trial of a new immunotherapy treatment called chimeric antigen receptor (CAR) T cell therapy. She was the first pediatric patient in the program.
Doctors took T cells from Emily’s blood and reprogrammed them in a lab. They essentially sent her T cells to boot camp where they are trained to find cancer cells and destroy them. The reprogrammed T cells were then injected back into her body. A week into treatment, she started getting a fever, the first sign that the treatment was working and her reprogrammed T cells were fighting the cancer. But soon, she got very sick. All of the indicators suggested that she had cytokine release syndrome (CRS)—also known as the cytokine storm. This happens when cytokines are released in response to an infection but the process cannot be turned off. The cytokines continue to attract immune cells to the infection site, causing damage to the patient’s own cells and eventually resulting in acute respiratory distress syndrome (ARDS). (Learn more about the cytokine storm in this blog.)
Emily was soon on a ventilator. Tests showed that she had extremely high levels of one particular cytokine: interleukin-6 (IL-6). Desperate to keep her alive, her doctors gave her a known drug that specifically targets IL-6. The results were dramatic. After one single dose, her fever subsided within hours, and she was taken off the ventilator. On May 2nd, 2012, she woke up from an induced coma—it was her 7th birthday. Her doctors said they have never seen a patient that sick get better that quickly.
In recent years, scientists have been hot on the trail of transcription factor FOXO3, tracing its involvement in various tumor-centric activities comprising the many trademarks of cancer, from drug resistance to metastasis to tumor angiogenesis.
FOXO3 is a member of the O sub-class of the forkhead box family of transcription factors. The forkhead box (FOX) family is characterized by a fork head DNA-binding domain (DBD), comprised of around 100 amino acids. They have also proven themselves to be a family of many hats, functioning in diverse roles ranging from metabolism, immunology, cell-cycle control, development, as well as cancer (1). The forkhead box O (FOXO) sub-class alone has demonstrated involvement in a variety of cellular outcomes, from drug resistance and longevity to apoptosis induction.
Due to its pro-apoptotic and anti-proliferative proclivity, FOXO3 has been previously identified as a tumor suppressor gene. However, more and more studies have begun to flip the narrative on FOXO3, portraying it more as a devoted henchman, due to its roles in drug and radiotherapy resistance, cell-cycle arrest and long-term maintenance of leukemia-initiating stem cells in a variety of cancer types, including breast cancer, pancreatic cancer, glioblastoma, and both acute and chronic myeloid leukemia.
XWe use cookies and similar technologies to make our website work, run analytics, improve our website, and show you personalized content and advertising. Some of these cookies are essential for our website to work. For others, we won’t set them unless you accept them. To learn more about our approach to Privacy we invite you to Read More
By clicking “Accept All”, you consent to the use of ALL the cookies. However you may visit Cookie Settings to provide a controlled consent.
We use cookies and similar technologies to make our website work, run analytics, improve our website, and show you personalized content and advertising. Some of these cookies are essential for our website to work. For others, we won’t set them unless you accept them. To find out more about cookies and how to manage cookies, read our Cookie Policy.
If you are located in the EEA, the United Kingdom, or Switzerland, you can change your settings at any time by clicking Manage Cookie Consent in the footer of our website.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-advertisement
1 year
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Advertisement".
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
gdpr_status
6 months 2 days
This cookie is set by the provider Media.net. This cookie is used to check the status whether the user has accepted the cookie consent box. It also helps in not showing the cookie consent box upon re-entry to the website.
lang
This cookie is used to store the language preferences of a user to serve up content in that stored language the next time user visit the website.
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Cookie
Duration
Description
SC_ANALYTICS_GLOBAL_COOKIE
10 years
This cookie is associated with Sitecore content and personalization. This cookie is used to identify the repeat visit from a single user. Sitecore will send a persistent session cookie to the web client.
vuid
2 years
This domain of this cookie is owned by Vimeo. This cookie is used by vimeo to collect tracking information. It sets a unique ID to embed videos to the website.
WMF-Last-Access
1 month 18 hours 24 minutes
This cookie is used to calculate unique devices accessing the website.
_ga
2 years
This cookie is installed by Google Analytics. The cookie is used to calculate visitor, session, campaign data and keep track of site usage for the site's analytics report. The cookies store information anonymously and assign a randomly generated number to identify unique visitors.
_gid
1 day
This cookie is installed by Google Analytics. The cookie is used to store information of how visitors use a website and helps in creating an analytics report of how the website is doing. The data collected including the number visitors, the source where they have come from, and the pages visted in an anonymous form.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.
Cookie
Duration
Description
IDE
1 year 24 days
Used by Google DoubleClick and stores information about how the user uses the website and any other advertisement before visiting the website. This is used to present users with ads that are relevant to them according to the user profile.
test_cookie
15 minutes
This cookie is set by doubleclick.net. The purpose of the cookie is to determine if the user's browser supports cookies.
VISITOR_INFO1_LIVE
5 months 27 days
This cookie is set by Youtube. Used to track the information of the embedded YouTube videos on a website.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Cookie
Duration
Description
YSC
session
This cookies is set by Youtube and is used to track the views of embedded videos.
_gat_UA-62336821-1
1 minute
This is a pattern type cookie set by Google Analytics, where the pattern element on the name contains the unique identity number of the account or website it relates to. It appears to be a variation of the _gat cookie which is used to limit the amount of data recorded by Google on high traffic volume websites.