Lynch Syndrome is the autosomal dominant hereditary predisposition to develop colorectal cancer and certain other cancers. This simple, one sentence definition seems woefully inadequate considering the human toll this condition has inflicted on the families that have it in their genetic pedigree.
They Called it a Curse
To one family, perhaps the family when it comes to this condition, Lynch Syndrome has meant heartache and hope; grief and joy; death and life. Their story is told by Ami McKay in her book Daughter of Family G, and it is at once both a memoir of a Lynch Syndrome previvor (someone with a Lynch Syndrome genomic mutation who has not yet developed cancer) and a poignant and honest account of the family that helped science put name to a curse.
“The doctors called it cancer. I say it’s a curse. I wish I knew what we did to deserve it.”
Anna Haab from Daughter of Family G (1)
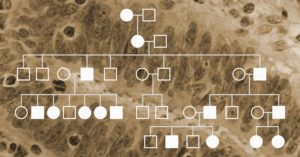
The scientific community first met “Family G” as the meticulously created family tree, filled with the stunted branches that mark early deaths by cancer. The pedigree was first published in 1913 in Archives of Internal Medicine (2). In the article, Dr. Alderd Warthin wrote: “A marked susceptibility to carcinoma exists in the case of certain family generations and family groups.” In 1925, an expanded pedigree of circles and squares was published in Dr. Warthin’s follow up study in the Journal of Cancer Research (3). But each circle and square in that pedigree denotes a person. Each line represents their dreams together for the future, and Ms. McKay wants us to know their names: Johannes and Anna, Kathrina, Elmer, Tillie, Sarah Anne (Sally); and—most importantly—Pauline. Because without Pauline there would be no story.
There are as many different
cancers as there are people with cancer. Unlike infectious diseases, which are
caused by pathogens that are foreign to our bodies (bacteria, viruses, parasites),
cancer cells arise from our body—our own cells gone rogue. Because cancer is a
dysfunction of a person’s normal cells, every cancer reflects the genetic
differences that mark us as individuals. Add to that environmental influences like
diet, tobacco use, the microbiome and even occupation, and the likelihood of
finding a “single” pharmaceutical cure for cancer becomes virtually impossible.
But, while looking for a single cure for all cancers may not be a fruitful activity, defining a best practice for understanding the genetic and protein biomarkers of individual tumors is proving worthwhile.
Lynch Syndrome is a hereditary condition caused by germline mutations that inactivate at least one of the major DNA mismatch repair (MMR) genes. Individuals with Lynch Syndrome have an elevated risk of developing several cancers, especially colorectal, uterine and endometrial. Approximately 1 in 279 individuals in the United States is Lynch-positive, but most people are unaware of their status.
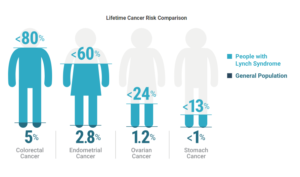
Lynch Syndrome results in highly elevated risks of several cancers.
Lynch Syndrome can be diagnosed following screening by microsatellite instability (MSI) analysis or immunohistochemistry (IHC) for the MMR proteins. For some patients, MMR gene sequencing is as easy as an oral “swish.” However, the genetic basis of Lynch Syndrome and its clinical relevancy are relatively recent discoveries. Long before modern sequencing methods simplified testing and diagnosis, a seamstress in Ann Arbor, Michigan correctly predicted her own Lynch Syndrome status based only on her family history. Talking with Dr. Alfred Scott Warthin in the late 19th century, she said that since so many of her family members had died of several specific cancers, she believed that she would follow the same path. Several years later, she unfortunately proved herself right.
Dr. Warthin took interest in the story and began studying the woman’s family. At the time of their conversation, five of her nine siblings had already been diagnosed with uterine, stomach or “abdominal” cancer. Warthin concluded that the family, which he dubbed “Cancer Family G,” did, in fact, have a predisposition to cancer. Warthin and other researchers continued studying the family for several decades. They found that cancers of the colon, uterus and stomach were most common, and that many members of the family were diagnosed at extraordinarily young ages.
In the 1970s, Dr. Henry T. Lynch organized a family reunion for Cancer Family G and subsequently published a report on “Cancer Family Syndrome.” By this time, 95 members of the family had developed one of the expected cancers. Dr. Lynch still didn’t have the technology to determine the molecular basis of the disease, but he noticed that it followed an autosomal dominant inheritance pattern.
In the mid-1990s, three labs simultaneously discovered microsatellite instability and its connection to colorectal cancer. It had been established in bacteria and yeast that inactivating mutations in DNA mismatch repair genes resulted in mutations in microsatellite sequences, so several labs began racing to clone the human homologs of the DNA MMR genes. Within a few months, two labs had cloned the MSH2 gene and found mutations that were present in members of Lynch-positive families who developed cancer.
Around this time, the name “Lynch Syndrome” was adopted to apply to families carrying germline mutations in a gene associated with the condition. Further research established four genes (MSH2, MLH1, MSH6, PMS2) as “Lynch Syndrome Genes,” and researchers began working on guidelines for diagnostic testing (See “The History of Lynch Syndrome” below for further reading).
Today, over two decades later, many researchers are pushing for the adoption of universal tumor screening for Lynch Syndrome. One of the widely recommended screening method is MSI analysis. MSI-H status indicates that certain sections of DNA called microsatellites have become unstable because the major mismatch repair genes that correct errors during DNA replication are not functioning properly. MSI status can influence treatment decisions, based on the 2015 discovery that MSI-H tumors respond well to immunotherapy drugs (1).
Lynch Syndrome awareness is also important knowledge for a patient’s family. Lynch-associated cancers are among the most preventable, so individuals who know they are Lynch-positive can work with their healthcare providers to develop robust strategies for prevention and surveillance. As one Lynch-positive mother said to her Lynch-positive son, “Your knowledge is power, and it’s going to keep you healthy and safe.”
Life with Lynch Syndrome: Read about what a Lynch Syndrome diagnosis means for Carrie Ketcham and her family
Dreaming of Universal Tumor Screening: Learn how cancer genetic counselor Heather Hampel is advocating for universal tumor screening and more Lynch Syndrome awareness
The History of Lynch Syndrome: Dr. C. Richard Boland and Dr. Henry T. Lynch provide a broad review of Lynch Syndrome research, starting over a hundred years ago.
The 2018 Nobel Prize in Physiology and Medicine was awarded to James P. Allison of the United States and Tasuku Honjo of Japan for their work to identify pathways in the immune system that can be used to attack cancer cells (1). Although immunotherapy for cancer has been a goal for many decades, Dr. Allison and Dr. Honjo succeeded through their manipulation of “checkpoint inhibitor” pathways to target cancer cells.
Immune checkpoint inhibitor drugs have been effective in cancers such as aggressive metastatic melanoma, some lung cancers, kidney, bladder and head and neck cancers. These therapies have succeeded in pushing many aggressive cancers below detectable limits, though these cases are notably not relapse-free or necessarily “cured” (2,3).
One challenge in implementing immunotherapy in a cancer treatment regime is the need to understand the genetic makeup of the tumor. Certain tumors, with specific genetic features, are far more likely to respond to immune checkpoint therapy than others. For this reason, Microsatellite Instability (MSI) analysis has become an increasingly relevant tool in genetic and immuno-oncology research.
XWe use cookies and similar technologies to make our website work, run analytics, improve our website, and show you personalized content and advertising. Some of these cookies are essential for our website to work. For others, we won’t set them unless you accept them. To learn more about our approach to Privacy we invite you to Read More
By clicking “Accept All”, you consent to the use of ALL the cookies. However you may visit Cookie Settings to provide a controlled consent.
We use cookies and similar technologies to make our website work, run analytics, improve our website, and show you personalized content and advertising. Some of these cookies are essential for our website to work. For others, we won’t set them unless you accept them. To find out more about cookies and how to manage cookies, read our Cookie Policy.
If you are located in the EEA, the United Kingdom, or Switzerland, you can change your settings at any time by clicking Manage Cookie Consent in the footer of our website.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-advertisement
1 year
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Advertisement".
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
gdpr_status
6 months 2 days
This cookie is set by the provider Media.net. This cookie is used to check the status whether the user has accepted the cookie consent box. It also helps in not showing the cookie consent box upon re-entry to the website.
lang
This cookie is used to store the language preferences of a user to serve up content in that stored language the next time user visit the website.
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Cookie
Duration
Description
SC_ANALYTICS_GLOBAL_COOKIE
10 years
This cookie is associated with Sitecore content and personalization. This cookie is used to identify the repeat visit from a single user. Sitecore will send a persistent session cookie to the web client.
vuid
2 years
This domain of this cookie is owned by Vimeo. This cookie is used by vimeo to collect tracking information. It sets a unique ID to embed videos to the website.
WMF-Last-Access
1 month 18 hours 24 minutes
This cookie is used to calculate unique devices accessing the website.
_ga
2 years
This cookie is installed by Google Analytics. The cookie is used to calculate visitor, session, campaign data and keep track of site usage for the site's analytics report. The cookies store information anonymously and assign a randomly generated number to identify unique visitors.
_gid
1 day
This cookie is installed by Google Analytics. The cookie is used to store information of how visitors use a website and helps in creating an analytics report of how the website is doing. The data collected including the number visitors, the source where they have come from, and the pages visted in an anonymous form.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.
Cookie
Duration
Description
IDE
1 year 24 days
Used by Google DoubleClick and stores information about how the user uses the website and any other advertisement before visiting the website. This is used to present users with ads that are relevant to them according to the user profile.
test_cookie
15 minutes
This cookie is set by doubleclick.net. The purpose of the cookie is to determine if the user's browser supports cookies.
VISITOR_INFO1_LIVE
5 months 27 days
This cookie is set by Youtube. Used to track the information of the embedded YouTube videos on a website.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Cookie
Duration
Description
YSC
session
This cookies is set by Youtube and is used to track the views of embedded videos.
_gat_UA-62336821-1
1 minute
This is a pattern type cookie set by Google Analytics, where the pattern element on the name contains the unique identity number of the account or website it relates to. It appears to be a variation of the _gat cookie which is used to limit the amount of data recorded by Google on high traffic volume websites.