Chimeric Antigen Recepter (CAR)-T cell therapy is a personalized immunotherapy that harnesses the patient’s own immune system to combat cancer. It is done by engineering the patient’s T cells to specifically target and attack cancer cells in their body, and it has shown great success in treating various blood cancers such as leukemia.
Treating solid tumors with CAR-T cells, however, has proved much more challenging. This is mainly because solid tumors contain a heterogeneous population of cells, expressing a variety of antigens—many of which are also expressed in healthy cells. Therefore, T cells targeting solid tumors could potentially attack healthy tissue, resulting in serious side effects. In addition, solid tumors create a hostile microenvironment that is difficult for CAR-T cells to infiltrate.
Oncologists, do you know your colorectal cancer patients’ MSI status?
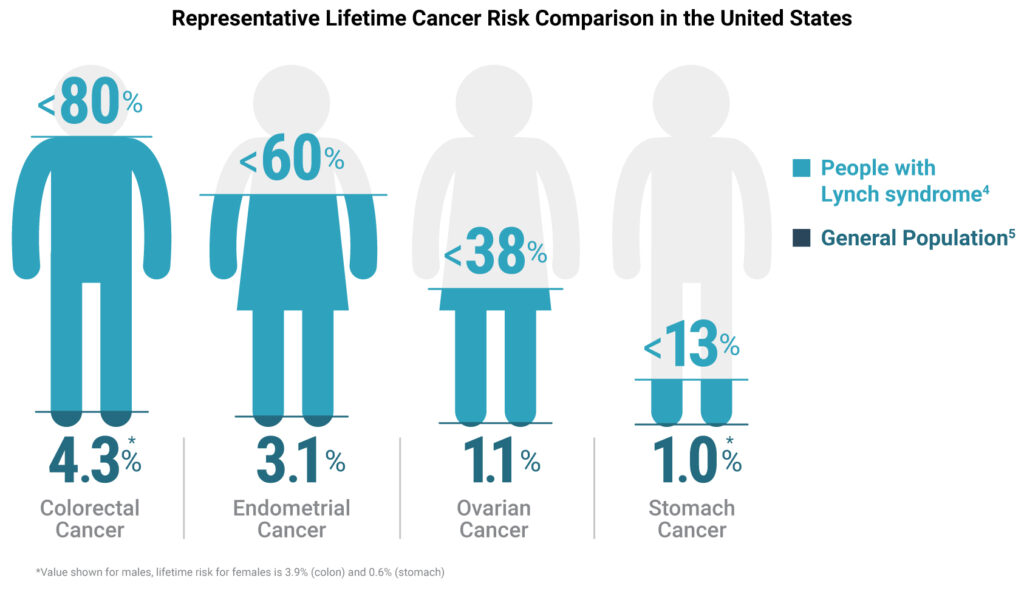
High-frequency microsatellite instability (MSI-H) in tumors is a form of genomic instability where mismatch repair (MMR) proteins fail to properly correct errors in microsatellite regions of the genome. When a patient’s tumor tissue is determined to have MSI-H markers, it’s strongly recommended that they be further tested for Lynch syndrome, a hereditary condition that puts them and their family at a higher risk of developing colorectal and other cancers (1).
Though as many as 1 in 279 people might be carriers for the mutations associated with Lynch syndrome (2), 95% of them don’t know it (3). Furthermore, people with Lynch syndrome have an approximately 80% increased lifetime risk of developing colorectal cancer, compared to a risk of only ~4% for the general population (4, 5).
On Lynch Syndrome Awareness Day, here are three key reasons why you should test all your colorectal cancer patients’ MSI status.
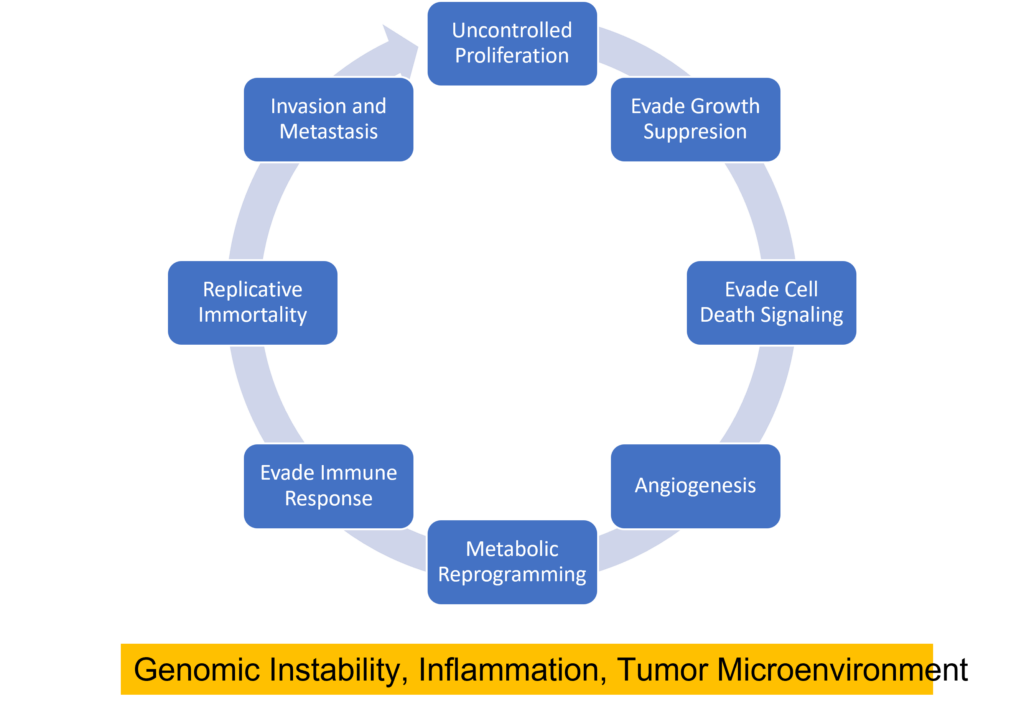
Cancer cells can be distinguished from normal cells by a variety of features including their ability to inappropriately activate signals for cell proliferation, evade growth suppression from contact inhibition or tumor suppressor activity, evade cell death signals, replicate DNA continually, induce angiogenesis, invade new tissues, reprogram their metabolism to provide energy for rapid proliferation, and evade immune detection (1) . Several biological processes are responsible for these features including genomic instability, inflammation, and the creation of a tumor microenvironment.
The tumor microenvironment is the network of non-malignant cells, connective tissue and blood vessels that surround and infiltrate the tumor. These surrounding “normal” cells interact with each other and the cancer cells and are important players in tumorigenesis. One cell type that is often found in the tumor microenvironment are nerve cells. In fact, cancer cells often express proteins that encourage nerve growth into the tumor microenvironment such as growth factors and axon-guidance molecules (2). Crosstalk between nerve cells and tumor cells can facilitate development of several cancer types (2) including pancreatic, head and neck, oral, prostate, and colorectal cancers.
Centrosaurus is a herbivorous Ceratopsian dinosaur that lived in Canada in the Cretaceous Period.
Did dinosaurs get cancer? That isn’t an easy question to answer. Finding and diagnosing cancer in dinosaur fossils has proven difficult. Any soft tissue, the typical location of tumors, has degraded over the millennia. Fossilized bones millions of years old are subject to wear and tear, making it hard to distinguish bone damage from possible pathology. By using the knowledge and expertise gained from diagnosing cancer in humans, a team reported in The Lancet Oncology that they found the first known case of osteosarcoma in a lower leg bone from a horned dinosaur found in southern Alberta, Canada.
This case of bone cancer discovered in a specimen of Centrosaurus apertus found in the Canadian Dinosaur Park Formation was confirmed by examining the bone surface along with radiographic and histological analysis. The 77–75.5-million-year-old case was compared to both a normal C. apertus fibula from the Oldman formation also in southern Alberta, Canada, as well as a human fibula with an osteosarcoma.
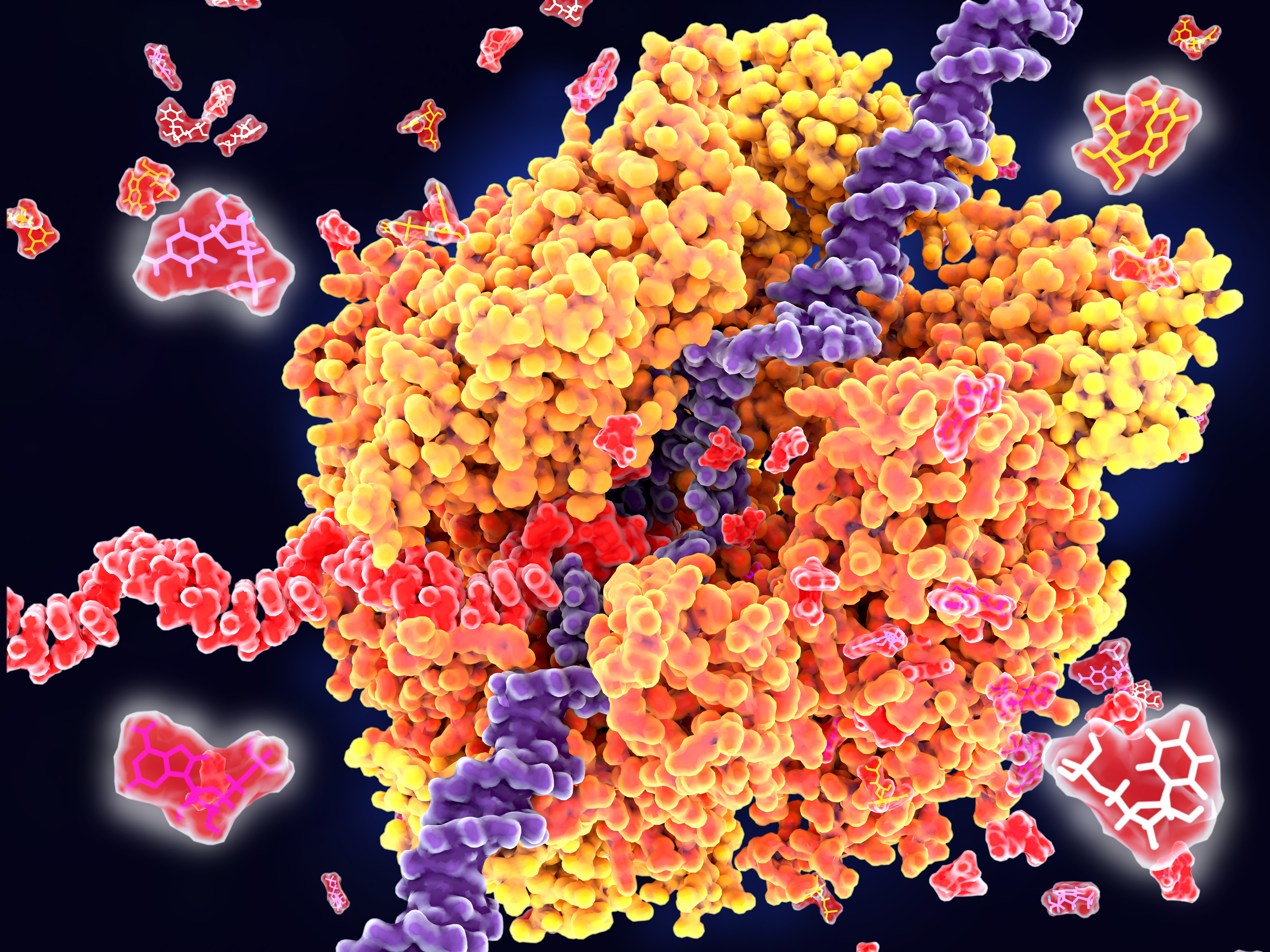
RNA polymerase unwinds DNA strands for transcription.
Transcription is the production of RNA from a DNA sequence. It’s a necessary life process in most cells. Transcription performed in vitro is also a valuable technique for research applications—from gene expression studies to the development of RNA virus vaccines.
During transcription, the DNA sequence is read by RNA polymerase to produce a complimentary, antiparallel RNA strand. This RNA strand is called a primary transcript, often referred to as an RNA transcript. In vitro transcription is a convenient method for generating RNA in a controlled environment outside of a cell.
In vitro transcription offers flexibility when choosing a DNA template, with a few requirements. The template must be purified, linear, and include a double stranded promoter region. Acceptable template types are plasmids or cloning vectors, PCR products, synthetic oligos (oligonucleotides), and cDNA (complimentary DNA).
In vitro transcription is used for production of large amounts of RNA transcripts for use in many applications including gene expression studies, RNA interference studies (RNAi), generation of guide RNA (gRNA) for use in CRISPR, creation of RNA standards for quantification of results in reverse-transcription quantitative PCR (RT-qPCR), studies of RNA structure and function, labeling of RNA probes for blotting and hybridization or for RNA:protein interaction studies, and preparation of specific cDNA libraries, just to name a few!
In vitro transcription can also be applied in general virology to study the effects of an RNA virus on a cell or an organism, and in development and production of RNA therapeutics and RNA virus vaccines. The large quantity of viral RNA produced through in vitro transcription can be used as inoculation material for viral infection studies. Viral mRNA transcripts, typically coding for a disease-specific antigen, can be quickly created through in vitro transcription, and used in the production of vaccines and therapeutics.
In 2012, a 6-year-old girl named Emily Whitehead was battling acute lymphoblastic leukemia (ALL), one of the most common cancers in children. Her cancer was stubborn. After 16 months of chemotherapy, the cancer still would not go into remission. There was nothing else the doctors could do, and she was sent home. She was expected to survive only a few more months. Her parents would not give up and enrolled her into a clinical trial of a new immunotherapy treatment called chimeric antigen receptor (CAR) T cell therapy. She was the first pediatric patient in the program.
Doctors took T cells from Emily’s blood and reprogrammed them in a lab. They essentially sent her T cells to boot camp where they are trained to find cancer cells and destroy them. The reprogrammed T cells were then injected back into her body. A week into treatment, she started getting a fever, the first sign that the treatment was working and her reprogrammed T cells were fighting the cancer. But soon, she got very sick. All of the indicators suggested that she had cytokine release syndrome (CRS)—also known as the cytokine storm. This happens when cytokines are released in response to an infection but the process cannot be turned off. The cytokines continue to attract immune cells to the infection site, causing damage to the patient’s own cells and eventually resulting in acute respiratory distress syndrome (ARDS). (Learn more about the cytokine storm in this blog.)
Emily was soon on a ventilator. Tests showed that she had extremely high levels of one particular cytokine: interleukin-6 (IL-6). Desperate to keep her alive, her doctors gave her a known drug that specifically targets IL-6. The results were dramatic. After one single dose, her fever subsided within hours, and she was taken off the ventilator. On May 2nd, 2012, she woke up from an induced coma—it was her 7th birthday. Her doctors said they have never seen a patient that sick get better that quickly.
In recent years, scientists have been hot on the trail of transcription factor FOXO3, tracing its involvement in various tumor-centric activities comprising the many trademarks of cancer, from drug resistance to metastasis to tumor angiogenesis.
FOXO3 is a member of the O sub-class of the forkhead box family of transcription factors. The forkhead box (FOX) family is characterized by a fork head DNA-binding domain (DBD), comprised of around 100 amino acids. They have also proven themselves to be a family of many hats, functioning in diverse roles ranging from metabolism, immunology, cell-cycle control, development, as well as cancer (1). The forkhead box O (FOXO) sub-class alone has demonstrated involvement in a variety of cellular outcomes, from drug resistance and longevity to apoptosis induction.
Due to its pro-apoptotic and anti-proliferative proclivity, FOXO3 has been previously identified as a tumor suppressor gene. However, more and more studies have begun to flip the narrative on FOXO3, portraying it more as a devoted henchman, due to its roles in drug and radiotherapy resistance, cell-cycle arrest and long-term maintenance of leukemia-initiating stem cells in a variety of cancer types, including breast cancer, pancreatic cancer, glioblastoma, and both acute and chronic myeloid leukemia.
Bacteria make you sick. The idea that bacteria cause illness has become ingrained in modern society, made evident by every sign requiring employees to wash their hands before leaving a restroom and the frequent food recalls resulting from pathogens like E. coli. But a parallel idea has also taken hold. As microbiome research continues to reveal the important role that bacteria play in human health, we’re starting to see the ways that the microbiota of the human body may be as important as our genes or environment.
The story of how our microbiome affects our health continues to get more complex. For example, researchers are now beginning to understand that the composition of bacteria residing in your body can significantly impact the effects of therapeutic drugs. This is a new factor for optimizing drug response, compared to other considerations such as diet, interaction with other drugs, administration time and comorbidity, which have been understood much longer.
When it comes to combating cancer does size matter? If every cell in the body has the propensity to become cancerous, it should naturally follow that larger animals that pack greater number of body cells and that those whose cells undergo greater number of cell divisions are more likely to develop cancer. By the same logic, organisms with longer lifespans must also have a greater chance of accumulating mutations leading to cancer. Surprisingly, the risk of developing cancer is only 5% in elephants and 18% in whales whereas it is as high as 30% in humans and rodents. The apparent lack of correlation between body mass, longevity and cancer- known as Peto’s paradox- has flummoxed scientists for several decades.1
A recent study published in Journal of the American Medical Association by Abegglen and colleagues has unlocked the secret weapon held by the pachyderms in fighting cancer2. While the weapon itself might not be new to cancer biologists, the stash carried by these marvelous animals is the highest recorded for any living species so far. To understand this weapon let’s revisit the coping mechanisms developed by cells to prevent cancer. When mammalian cells are exposed to cancer inducing treatments, such as UV radiation for example, a gene encoding TP53, kicks into gear making copies of the tumor suppressing protein of the same name. TP53 acts as a tumor suppressor, which means that it regulates cell division by keeping cells from growing and dividing too fast or in an uncontrolled way. It does so by either repairing any damage to the cells caused by the UV exposure or by killing off the cell by a self-destructing mechanism known as apoptosis which is akin to committing suicide.
Many mammals, including humans carry only two copies of this important gene; one copy or allele is inherited from each parent. If the TP53 gene is inactivated by mutations, the risk of developing cancer increases by several fold. A rare but lethal condition called Li-Fraumeni Syndrome marks patients who have only one working copy of TP53 with more than a 90 percent lifetime cancer risk from childhood into their adult years. In a quest to investigate the unexplained resistance to cancer by elephants, the scientists combed through the elephant genome and stumbled upon 40 copies of genes that code for TP53. One pair was ancestral in origin, whereas the remainder appear to have diverged from the ancestral copy and were archived within the genome over the course of evolution as retrogenes. Continue reading “Beating the Odds of Cancer: Not Just a Tall Tale”
The cover of S. Mukerjee’s book, The Emporer of All Maladies: The Biology of Cancer. Used courtesy of Wikimedia and WLU.
Dr. Drew M. Pardoll, Johns Hopkins University School of Medicine in Baltimore, in his 2012 review, “The blockade of immune checkpoints in cancer immunotherapy” published in Nature Reviews Cancer (1) writes:
“The myriad of genetic and epigenetic alterations that are characteristic of all cancers provide a diverse set of antigens that the immune system can use to distinguish tumour cells from their normal counterparts.”
Tumors have antigens, so we should be able to address/attack these antigens with our immune system, right?
Various immune mediators as therapeutic agents against cancer have entered and mostly flopped in clinical trials over the past 30 or more years. As a graduate student in the 1980s I remember IL-2 and interferon raising many hopes. More recently, drugs against chronic myeloid leukemia and CLL have shown early promise. However, so far cancer cells have mostly won against these therapies. Yet recent news points to some exciting new therapeutic agents, that over the past 15 years or so, and in and out of clinical trials, are getting a leg up in the cancer battle. These drugs are immune checkpoint inhibitors.
XWe use cookies and similar technologies to make our website work, run analytics, improve our website, and show you personalized content and advertising. Some of these cookies are essential for our website to work. For others, we won’t set them unless you accept them. To learn more about our approach to Privacy we invite you to Read More
By clicking “Accept All”, you consent to the use of ALL the cookies. However you may visit Cookie Settings to provide a controlled consent.
We use cookies and similar technologies to make our website work, run analytics, improve our website, and show you personalized content and advertising. Some of these cookies are essential for our website to work. For others, we won’t set them unless you accept them. To find out more about cookies and how to manage cookies, read our Cookie Policy.
If you are located in the EEA, the United Kingdom, or Switzerland, you can change your settings at any time by clicking Manage Cookie Consent in the footer of our website.
Necessary cookies are absolutely essential for the website to function properly. These cookies ensure basic functionalities and security features of the website, anonymously.
Cookie
Duration
Description
cookielawinfo-checbox-analytics
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Analytics".
cookielawinfo-checbox-functional
11 months
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Functional".
cookielawinfo-checbox-others
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Other.
cookielawinfo-checkbox-advertisement
1 year
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Advertisement".
cookielawinfo-checkbox-necessary
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookies is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-performance
11 months
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Performance".
gdpr_status
6 months 2 days
This cookie is set by the provider Media.net. This cookie is used to check the status whether the user has accepted the cookie consent box. It also helps in not showing the cookie consent box upon re-entry to the website.
lang
This cookie is used to store the language preferences of a user to serve up content in that stored language the next time user visit the website.
viewed_cookie_policy
11 months
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
Analytical cookies are used to understand how visitors interact with the website. These cookies help provide information on metrics the number of visitors, bounce rate, traffic source, etc.
Cookie
Duration
Description
SC_ANALYTICS_GLOBAL_COOKIE
10 years
This cookie is associated with Sitecore content and personalization. This cookie is used to identify the repeat visit from a single user. Sitecore will send a persistent session cookie to the web client.
vuid
2 years
This domain of this cookie is owned by Vimeo. This cookie is used by vimeo to collect tracking information. It sets a unique ID to embed videos to the website.
WMF-Last-Access
1 month 18 hours 24 minutes
This cookie is used to calculate unique devices accessing the website.
_ga
2 years
This cookie is installed by Google Analytics. The cookie is used to calculate visitor, session, campaign data and keep track of site usage for the site's analytics report. The cookies store information anonymously and assign a randomly generated number to identify unique visitors.
_gid
1 day
This cookie is installed by Google Analytics. The cookie is used to store information of how visitors use a website and helps in creating an analytics report of how the website is doing. The data collected including the number visitors, the source where they have come from, and the pages visted in an anonymous form.
Advertisement cookies are used to provide visitors with relevant ads and marketing campaigns. These cookies track visitors across websites and collect information to provide customized ads.
Cookie
Duration
Description
IDE
1 year 24 days
Used by Google DoubleClick and stores information about how the user uses the website and any other advertisement before visiting the website. This is used to present users with ads that are relevant to them according to the user profile.
test_cookie
15 minutes
This cookie is set by doubleclick.net. The purpose of the cookie is to determine if the user's browser supports cookies.
VISITOR_INFO1_LIVE
5 months 27 days
This cookie is set by Youtube. Used to track the information of the embedded YouTube videos on a website.
Performance cookies are used to understand and analyze the key performance indexes of the website which helps in delivering a better user experience for the visitors.
Cookie
Duration
Description
YSC
session
This cookies is set by Youtube and is used to track the views of embedded videos.
_gat_UA-62336821-1
1 minute
This is a pattern type cookie set by Google Analytics, where the pattern element on the name contains the unique identity number of the account or website it relates to. It appears to be a variation of the _gat cookie which is used to limit the amount of data recorded by Google on high traffic volume websites.



 When it comes to combating cancer does size matter? If every cell in the body has the propensity to become cancerous, it should naturally follow that larger animals that pack greater number of body cells and that those whose cells undergo greater number of cell divisions are more likely to develop cancer. By the same logic, organisms with longer lifespans must also have a greater chance of accumulating mutations leading to cancer. Surprisingly, the risk of developing cancer is only 5% in elephants and 18% in whales whereas it is as high as 30% in humans and rodents. The apparent lack of correlation between body mass, longevity and cancer- known as Peto’s paradox- has flummoxed scientists for several decades.1
When it comes to combating cancer does size matter? If every cell in the body has the propensity to become cancerous, it should naturally follow that larger animals that pack greater number of body cells and that those whose cells undergo greater number of cell divisions are more likely to develop cancer. By the same logic, organisms with longer lifespans must also have a greater chance of accumulating mutations leading to cancer. Surprisingly, the risk of developing cancer is only 5% in elephants and 18% in whales whereas it is as high as 30% in humans and rodents. The apparent lack of correlation between body mass, longevity and cancer- known as Peto’s paradox- has flummoxed scientists for several decades.1